ANSYS Fluent for Hemodynamic Simulation: Modeling Blood Flow in Cardiovascular Devices
Computational fluid dynamics (CFD) has become an indispensable tool in cardiovascular device development. Among the available solvers, ANSYS Fluent stands out for its ability to model the complex, non-Newtonian, pulsatile flow conditions found in the human circulatory system. This article examines how biomedical engineers use Fluent to simulate hemodynamics in devices such as heart valves, ventricular assist devices (VADs), and coronary stents — and how these simulations feed directly into FDA regulatory submissions.
Why CFD Matters for Cardiovascular Devices
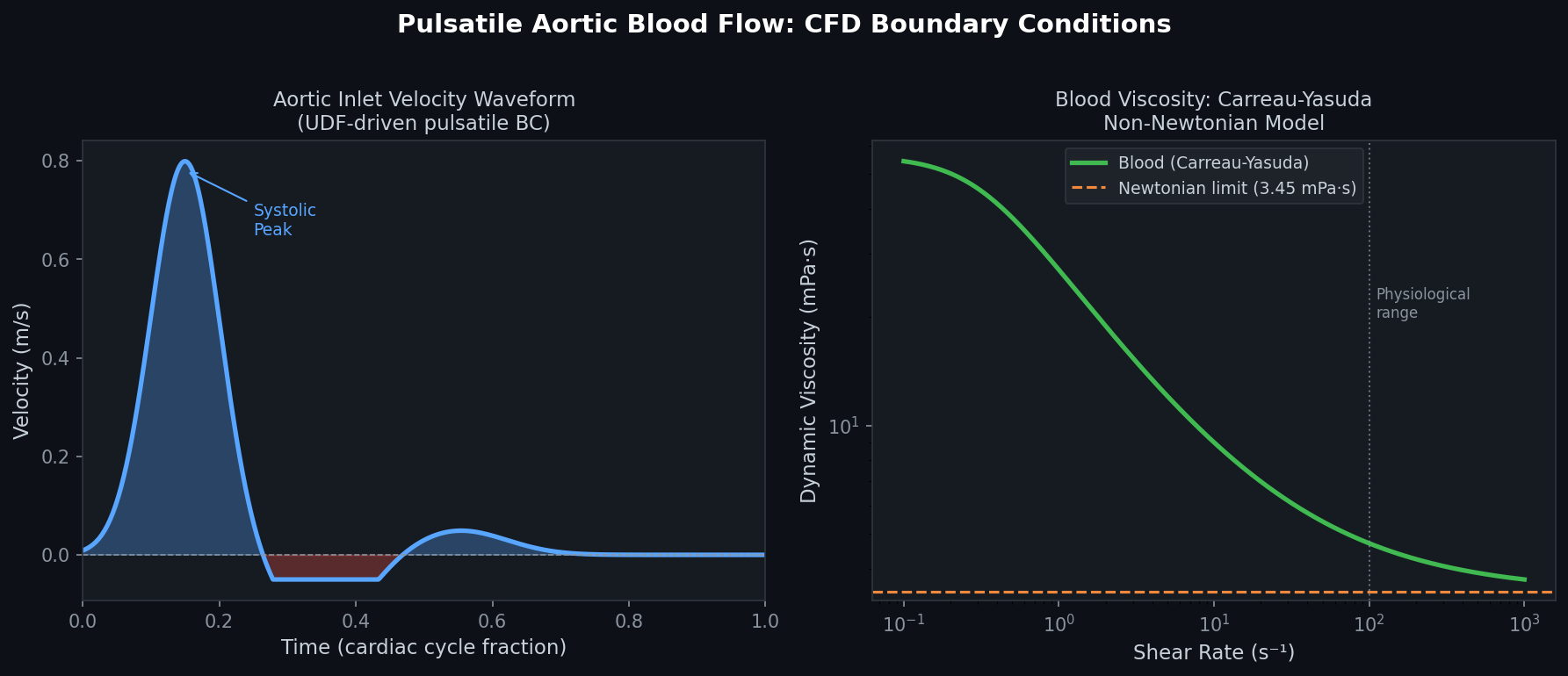
Blood is not a simple Newtonian fluid. At low shear rates (below ~100 s⁻¹), red blood cells aggregate into rouleaux structures, causing viscosity to rise sharply. At high shear rates, the fluid thins. This shear-thinning behavior must be captured accurately to predict:
- Wall shear stress (WSS) — low WSS promotes platelet adhesion and thrombosis; high WSS causes hemolysis.
- Recirculation zones — stagnant flow regions accelerate clot formation.
- Pressure drops — critical for sizing pumps and evaluating stenosis severity.
ANSYS Fluent supports multiple non-Newtonian viscosity models out of the box, including the Carreau-Yasuda and Power Law models, both widely used in peer-reviewed hemodynamics literature and accepted by the FDA's guidance on computational modeling (FDA-2016-D-2343).

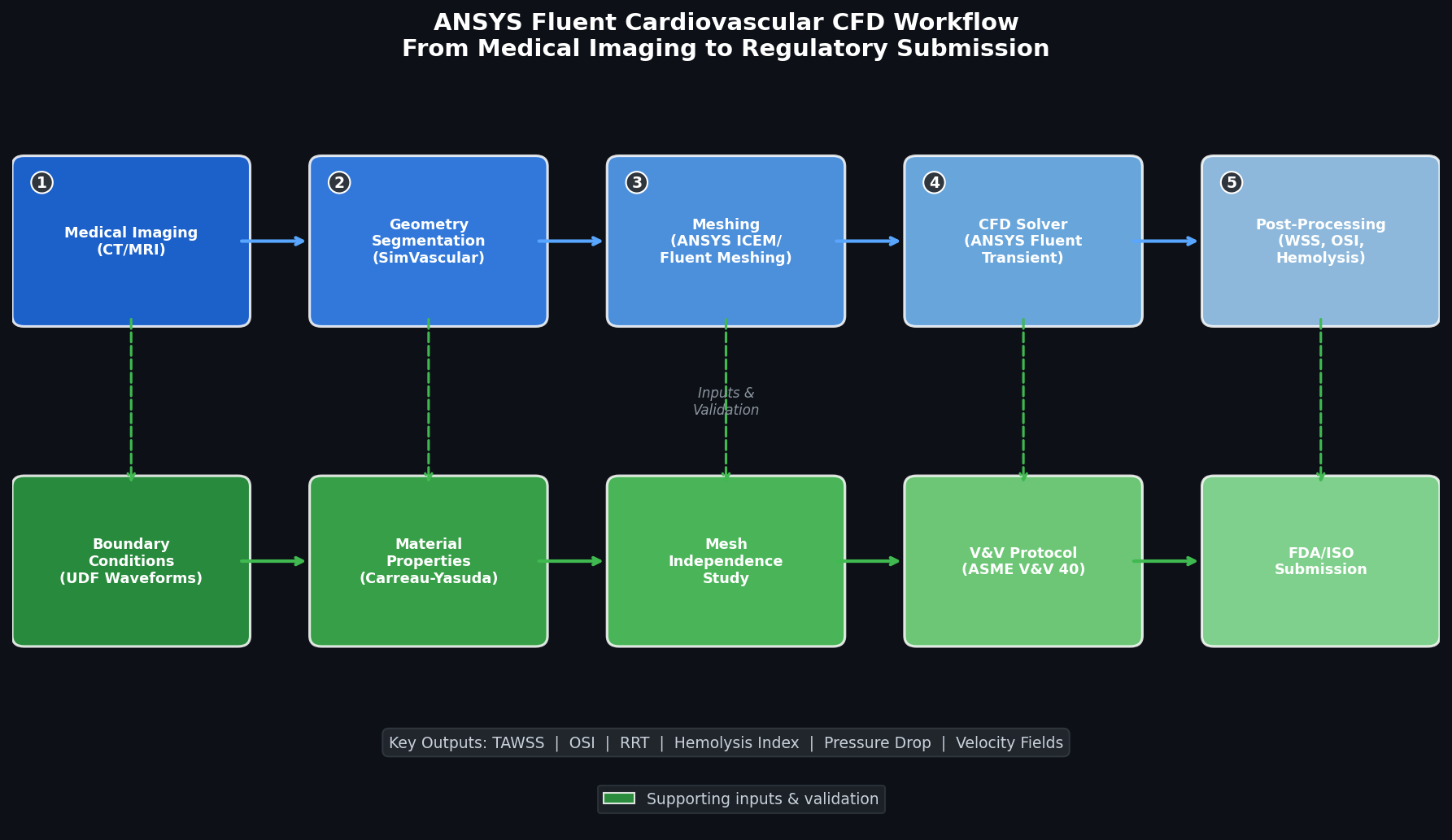
Setting Up a Hemodynamic Simulation in Fluent
1. Geometry and Meshing
Cardiovascular geometries are typically reconstructed from patient CT or MRI data using segmentation tools such as SimVascular or 3D Slicer, then imported into ANSYS SpaceClaim or ICEM CFD for cleanup. Key meshing considerations include:
- Boundary layer inflation: At least 5–8 prismatic layers at vessel walls to resolve the near-wall velocity gradient accurately. A y⁺ value below 1 is recommended for low-Reynolds-number flows.
- Polyhedral or tetrahedral core: Polyhedral meshes reduce cell count by 3–5× compared to tetrahedral meshes for equivalent accuracy, cutting solve time significantly.
- Mesh independence study: Always run at least three mesh densities (coarse, medium, fine) and verify that WSS and pressure drop change by less than 5% between the two finest levels.
2. Boundary Conditions
Physiologically realistic boundary conditions are essential:
- Inlet: Time-varying velocity profile derived from Doppler ultrasound or phase-contrast MRI waveforms. Fluent's User-Defined Functions (UDFs) allow direct import of waveform data as a C function, enabling patient-specific pulsatile inlet conditions.
- Outlet: Windkessel (three-element RCR) models are implemented via UDFs to represent downstream vascular resistance and compliance, avoiding the non-physiological flat-pressure assumption.
- Walls: Rigid-wall assumption is standard for metallic devices (stents, valve frames). For compliant vessels, Fluent's System Coupling module links to ANSYS Mechanical for fluid-structure interaction (FSI), capturing wall motion and its effect on flow.
3. Solver Settings
For pulsatile cardiovascular flows:
- Transient solver with a time step of 1–5 ms (corresponding to 200–1000 steps per cardiac cycle at 60 bpm).
- Pressure-based coupled solver for incompressible flow — faster convergence than the segregated SIMPLE algorithm for these geometries.
- Second-order temporal and spatial discretization to minimize numerical diffusion.
- Run at least 3 cardiac cycles before collecting data to eliminate initial transient effects; report results from the final cycle.
Key Output Metrics and Post-Processing
Fluent's post-processing environment (or export to EnSight/ParaView) enables extraction of the metrics most relevant to device safety:
| Metric | Clinical Relevance | Fluent Output |
|---|---|---|
| Time-averaged WSS (TAWSS) | Thrombosis risk (low WSS < 0.4 Pa) | Surface integral, cycle-averaged |
| Oscillatory Shear Index (OSI) | Disturbed flow, atherogenesis | Custom field function |
| Relative Residence Time (RRT) | Combined thrombosis indicator | Derived from TAWSS + OSI |
| Scalar Shear Stress (SSS) | Hemolysis prediction | Volume integral |
| Pressure drop (ΔP) | Device performance, sizing | Report → Surface integrals |
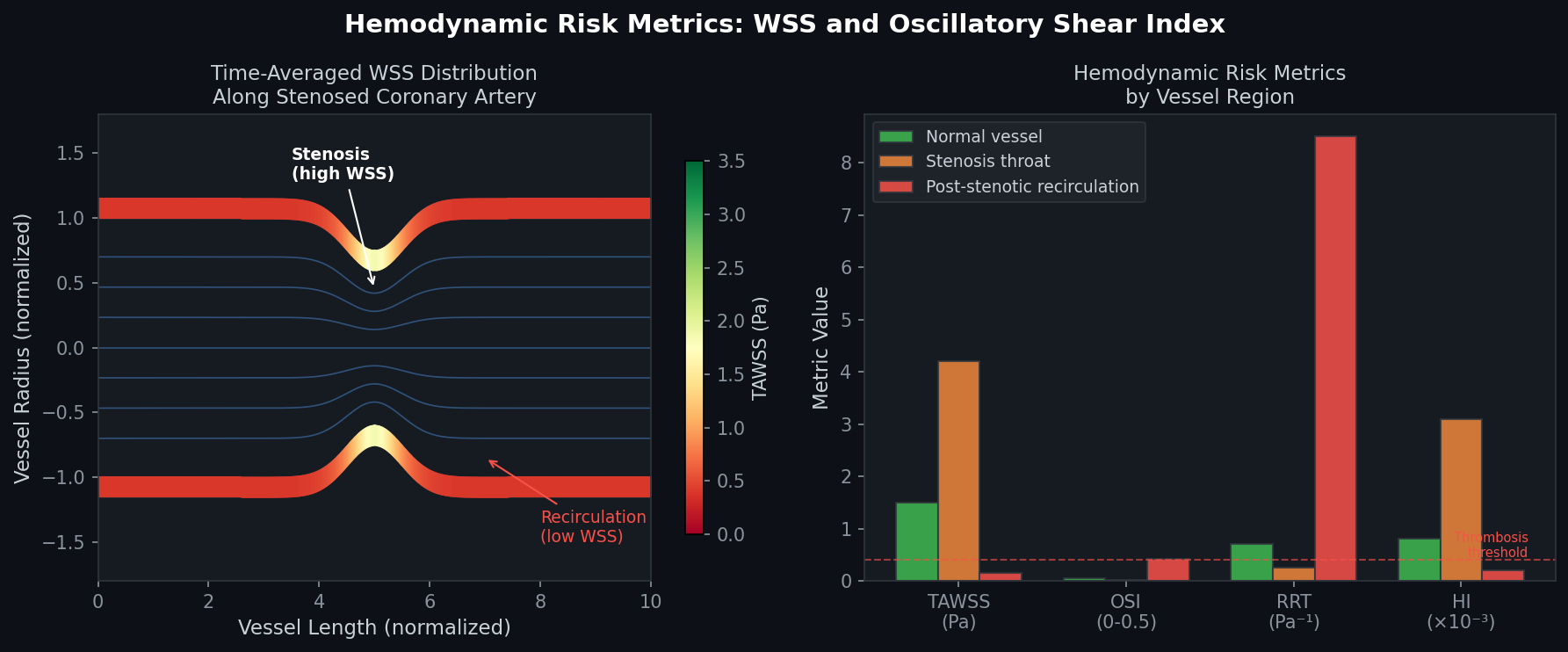
The Hemolysis Index (HI) — a measure of red blood cell damage — can be computed using power-law damage models (Giersiepen, Zhang) implemented as Fluent species transport equations or via post-processing scripts.
Regulatory Pathway: FDA and ISO 10993
The FDA's 2022 guidance "Reporting of Computational Modeling Studies in Medical Device Submissions" explicitly recognizes CFD as a valid tool for demonstrating device safety when accompanied by:
- Verification: Mesh independence, solver convergence, and comparison to analytical solutions.
- Validation: Experimental comparison using particle image velocimetry (PIV) or laser Doppler anemometry (LDA) in benchtop flow phantoms.
- Uncertainty Quantification (UQ): Sensitivity analysis on boundary conditions and material properties. Fluent's Design Exploration module (via ANSYS Workbench) automates parametric sweeps for UQ.
ISO 10993-4 (biological evaluation of blood-contacting devices) and ASTM F2996 (hemolysis testing) provide the experimental benchmarks against which CFD predictions are validated.
Practical Tips for Biomedical CFD Engineers
- Use double precision: Cardiovascular pressure differences are small relative to absolute pressures; single-precision arithmetic introduces unacceptable rounding errors.
- Monitor residuals AND physical quantities: Residuals alone are insufficient convergence criteria. Track inlet flow rate, outlet pressure, and a representative WSS value each time step.
- Leverage HPC: A typical coronary stent model with ~5 million cells and 1000 time steps requires 8–16 CPU cores and 6–12 hours. ANSYS Fluent scales efficiently to 256+ cores via MPI.
- Document everything: FDA reviewers expect complete documentation of geometry sources, mesh statistics, boundary condition derivation, and solver settings. Maintain a simulation log from day one.
Further Resources
- ANSYS Fluent User's Guide – Non-Newtonian Viscosity Models
- FDA Guidance: Reporting of Computational Modeling Studies in Medical Device Submissions (2022)
- SimVascular Open-Source Cardiovascular Simulation Platform
- ASME V&V 40 – Assessing Credibility of Computational Modeling in Medical Devices
- Journal of Biomechanical Engineering – CFD in Cardiovascular Devices
ANSYS Fluent's combination of non-Newtonian fluid models, UDF-driven physiological boundary conditions, FSI coupling, and robust HPC scalability makes it the solver of choice for regulatory-grade cardiovascular device hemodynamics. When paired with rigorous V&V protocols aligned to FDA and ASME standards, CFD simulations can meaningfully reduce animal testing, accelerate design iteration, and strengthen 510(k) and PMA submissions.