GastroPlus ACAT Model: Predicting Oral Drug Bioavailability with Mechanistic Absorption Simulation
Oral bioavailability is one of the most critical — and most unpredictable — parameters in drug development. A compound may show excellent potency in vitro yet fail in vivo because of poor solubility, slow dissolution, or limited intestinal permeability. GastroPlus (Simulations Plus, Inc.) addresses this challenge head-on with its Advanced Compartmental Absorption and Transit (ACAT) model, a mechanistic simulation framework that has become an industry standard for predicting oral drug absorption in humans and preclinical species.
What Is the ACAT Model?
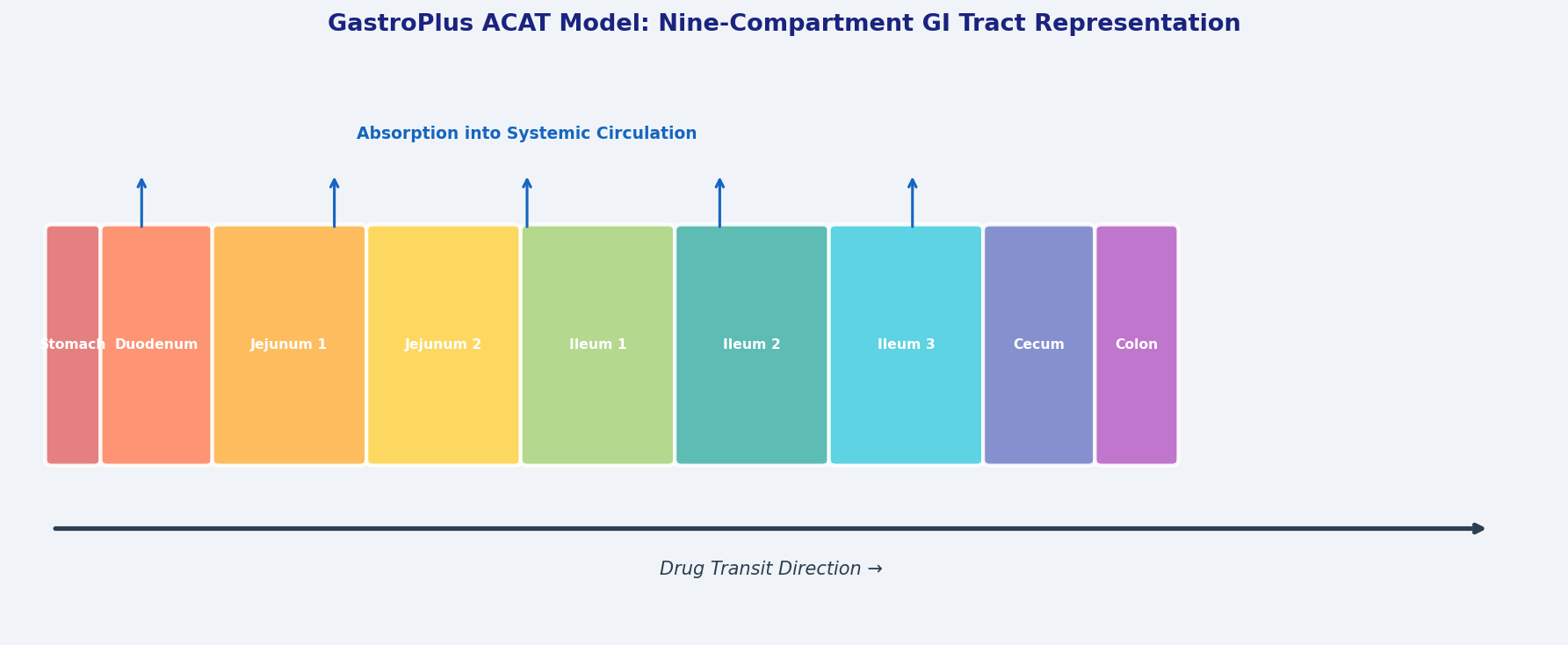
The ACAT model divides the gastrointestinal (GI) tract into nine physiologically distinct compartments — stomach, duodenum, two jejunal segments, three ileal segments, cecum, and ascending colon — each characterized by its own pH, transit time, fluid volume, bile salt concentration, and absorptive surface area. Drug dissolution, solubilization, and permeation are computed dynamically within each compartment as the virtual bolus moves through the tract.
Unlike empirical curve-fitting approaches, ACAT is mechanistic: it uses first-principles equations for dissolution (based on the Noyes–Whitney equation), passive and active transport, gut-wall metabolism (CYP3A4, P-gp efflux), and hepatic first-pass extraction. This mechanistic foundation means the model can extrapolate beyond the training data — a critical advantage when predicting behavior in fed versus fasted states, in special populations, or for novel formulations.

Setting Up a GastroPlus Simulation
A typical GastroPlus workflow for a new chemical entity (NCE) proceeds through four stages:
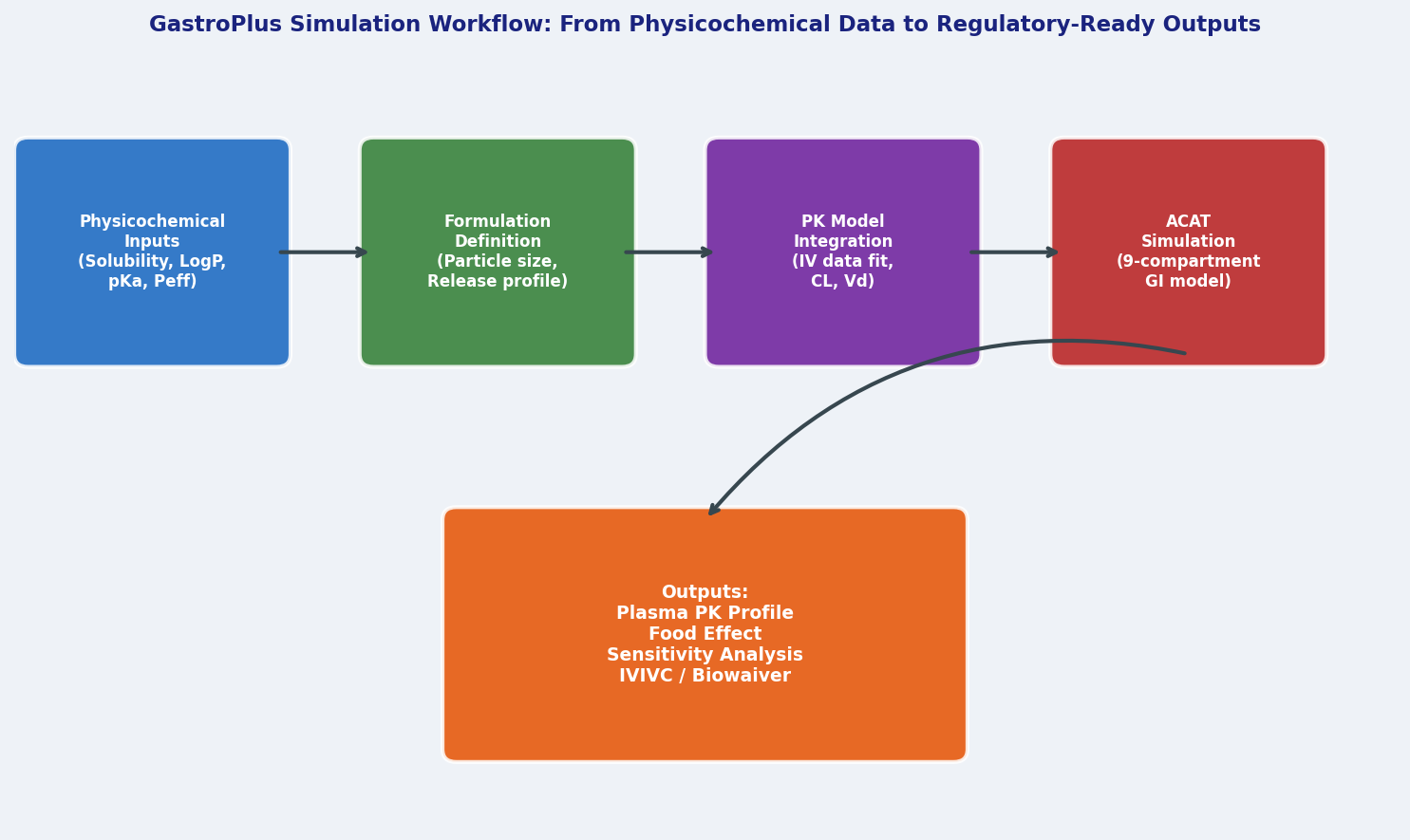
1. Physicochemical Input
The simulation requires measured or predicted values for:
- Solubility (pH-dependent, if ionizable)
- LogP / LogD (lipophilicity)
- pKa (ionization constants)
- Effective permeability (Peff) — ideally from Caco-2 or PAMPA assays, or estimated via the built-in ADMET Predictor module
GastroPlus accepts solubility as a single value or as a full pH–solubility profile, which is essential for weak acids and bases whose solubility changes dramatically across the GI pH gradient.
2. Formulation Definition
The formulation module allows users to specify particle size distribution, density, and dissolution medium for immediate-release (IR) tablets, capsules, or suspensions. For modified-release (MR) formulations, GastroPlus includes a dedicated IVIVC (In Vitro–In Vivo Correlation) module that links dissolution apparatus data (USP II paddle, USP IV flow-through cell) to in vivo absorption profiles, enabling Level A IVIVC development for regulatory submissions.
3. PK Model Integration
GastroPlus couples the absorption model to a compartmental pharmacokinetic (PK) model — typically a 1- or 2-compartment model parameterized with IV data. The software automatically fits systemic PK parameters (clearance, volume of distribution) from observed plasma concentration–time data, then uses those parameters to simulate oral PK profiles. This integrated PBPK-absorption approach is more predictive than treating absorption and disposition independently.
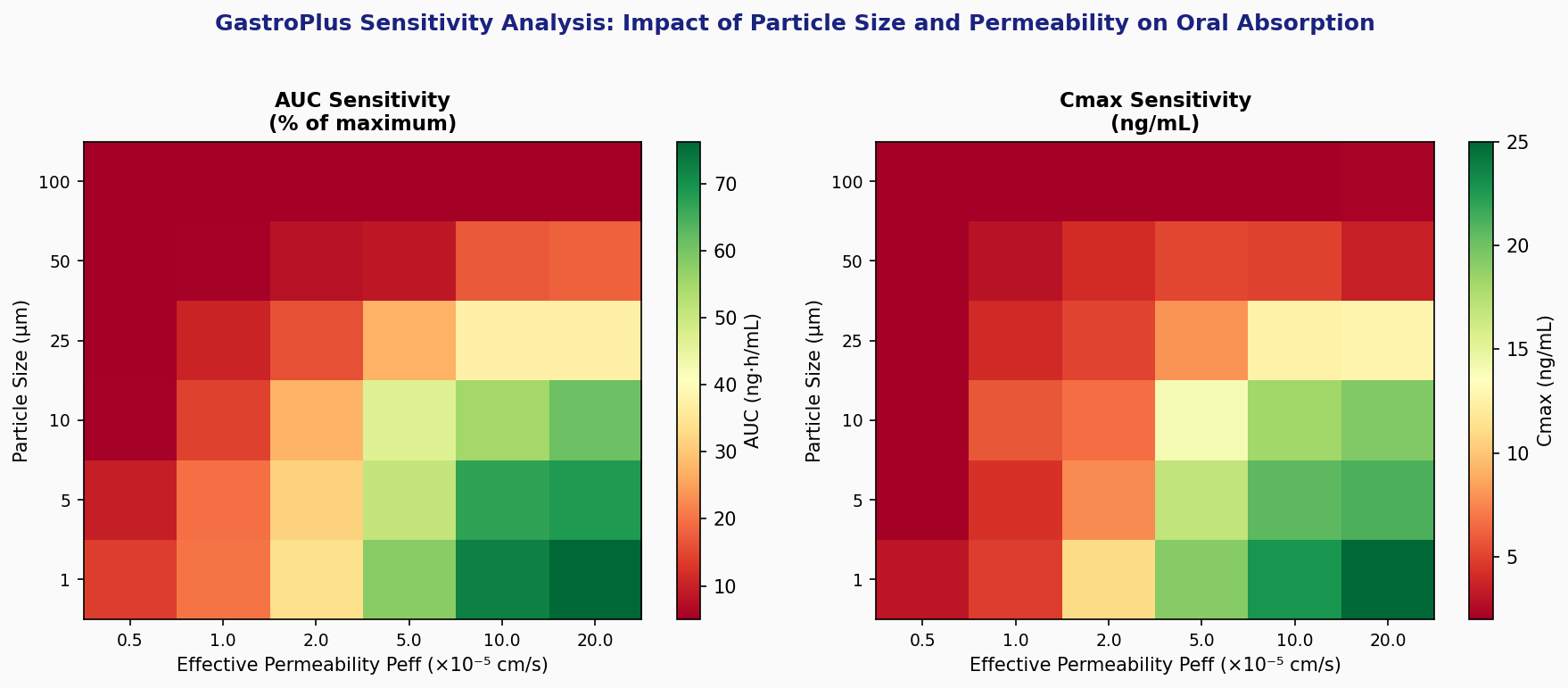
4. Simulation and Sensitivity Analysis
Once configured, a simulation runs in seconds. The Sensitivity Analysis tool is particularly powerful: it sweeps one or two input parameters (e.g., particle size from 1–100 µm, or Peff from 1×10⁻⁵ to 1×10⁻⁴ cm/s) across a defined range and plots the resulting Cmax and AUC values. This immediately reveals which physicochemical properties are rate-limiting for absorption — guiding formulation scientists toward the highest-leverage optimization targets.
Fed/Fasted State Prediction
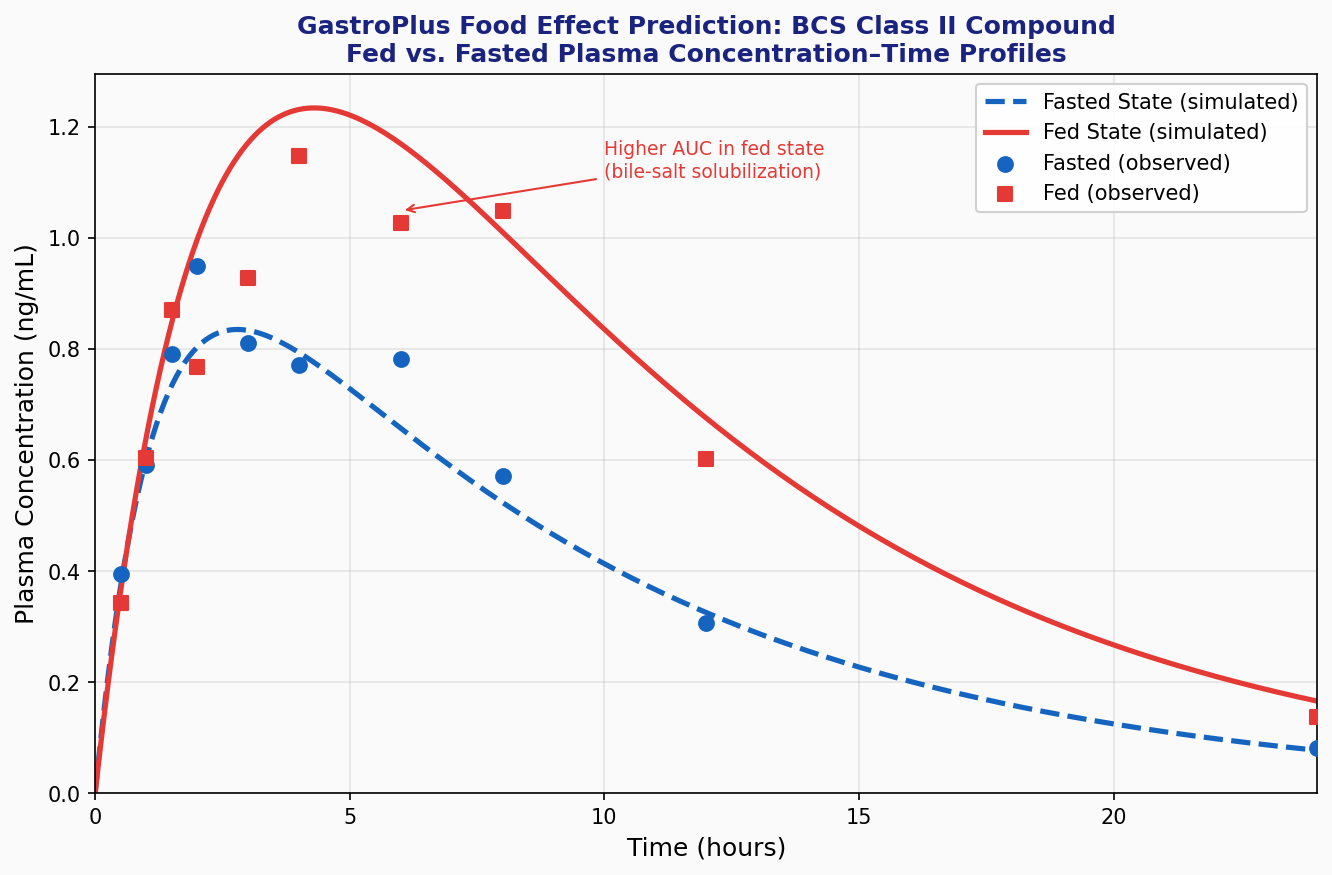
One of GastroPlus's most clinically relevant capabilities is its food effect prediction. The software ships with validated physiological parameter sets for both fasted and fed states (based on published biorelevant media data), and can simulate the impact of a high-fat meal on drug absorption. For BCS Class II compounds (low solubility, high permeability), the model correctly predicts the positive food effect driven by bile-salt-mediated solubilization and delayed gastric emptying. For BCS Class III compounds (high solubility, low permeability), it captures the negative food effect from reduced intestinal transit time.
This capability is directly applicable to regulatory strategy: FDA and EMA guidance on biowaivers and food-effect studies increasingly accept mechanistic PBPK/absorption modeling as supporting evidence, reducing the need for expensive clinical food-effect studies.
Population Variability and Virtual Clinical Trials
GastroPlus integrates with the PEAR (Population Estimates for Age-Related) physiology module, which provides age-, sex-, and weight-stratified GI physiological parameters. Combined with Monte Carlo sampling of PK variability, this enables virtual clinical trials — simulating plasma concentration profiles across hundreds of virtual subjects to predict the population distribution of Cmax and AUC. This is particularly valuable for pediatric formulation development, where clinical data are scarce and ethical constraints limit study designs.
Regulatory Acceptance and Industry Use
GastroPlus simulations are accepted by the FDA, EMA, and PMDA as supporting data in IND, NDA, and ANDA submissions. Common regulatory applications include:
- Biowaiver requests for BCS Class I and III compounds
- IVIVC development for modified-release formulations
- Food-effect risk assessment to justify waiving clinical food-effect studies
- Pediatric extrapolation of adult PK data
The software's validation database — comprising hundreds of published compounds with known human PK — provides confidence that predictions are within a 2-fold error for most drug classes.
Practical Tips for Accurate Predictions
- Use measured solubility, not predicted. Solubility is the single most influential input for BCS Class II drugs; computational predictions can be off by orders of magnitude.
- Calibrate Peff with in vitro data. The built-in ADMET Predictor estimates are useful for screening but should be replaced with Caco-2 data when available.
- Fit systemic PK from IV data first. Decoupling absorption from disposition reduces parameter correlation and improves identifiability.
- Run sensitivity analysis before optimization. Knowing which parameter dominates absorption efficiency prevents wasted formulation effort.
- Validate against at least one observed clinical profile before using the model for regulatory submissions.
Further Resources
- GastroPlus Official Documentation — product overview, validation reports, and regulatory submission examples
- FDA Guidance on PBPK Modeling — regulatory framework for mechanistic absorption and PBPK models
- EMA Guideline on PBPK — European regulatory expectations
- Simulations Plus IVIVC White Paper — practical guide to Level A IVIVC development with GastroPlus
- BCS Classification and Biowaivers (WHO) — foundational framework for biopharmaceutics classification
GastroPlus occupies a unique niche in the pharmaceutical simulation landscape: it bridges the gap between in vitro dissolution data and in vivo clinical outcomes with mechanistic rigor. For formulation scientists and clinical pharmacologists working on oral drug products, mastering the ACAT model is an investment that pays dividends across the entire development lifecycle — from lead optimization through regulatory submission.