Varian Eclipse TPS: Monte Carlo-Class Dose Calculation with Acuros XB for Lung SBRT
Varian Eclipse TPS: Monte Carlo Dose Calculation for Radiation Therapy Treatment Planning
Radiation therapy is one of the most physics-intensive disciplines in clinical medicine. Delivering a lethal dose to a tumor while sparing surrounding healthy tissue requires simulation accuracy measured in millimeters and fractions of a percent. Varian's Eclipse Treatment Planning System (TPS) is the industry-leading platform for this challenge, and its Acuros XB algorithm—a deterministic Linear Boltzmann Transport Equation (LBTE) solver—brings Monte Carlo–class accuracy to clinical workflows without the prohibitive computation times of full stochastic simulation.
Why Dose Calculation Accuracy Matters
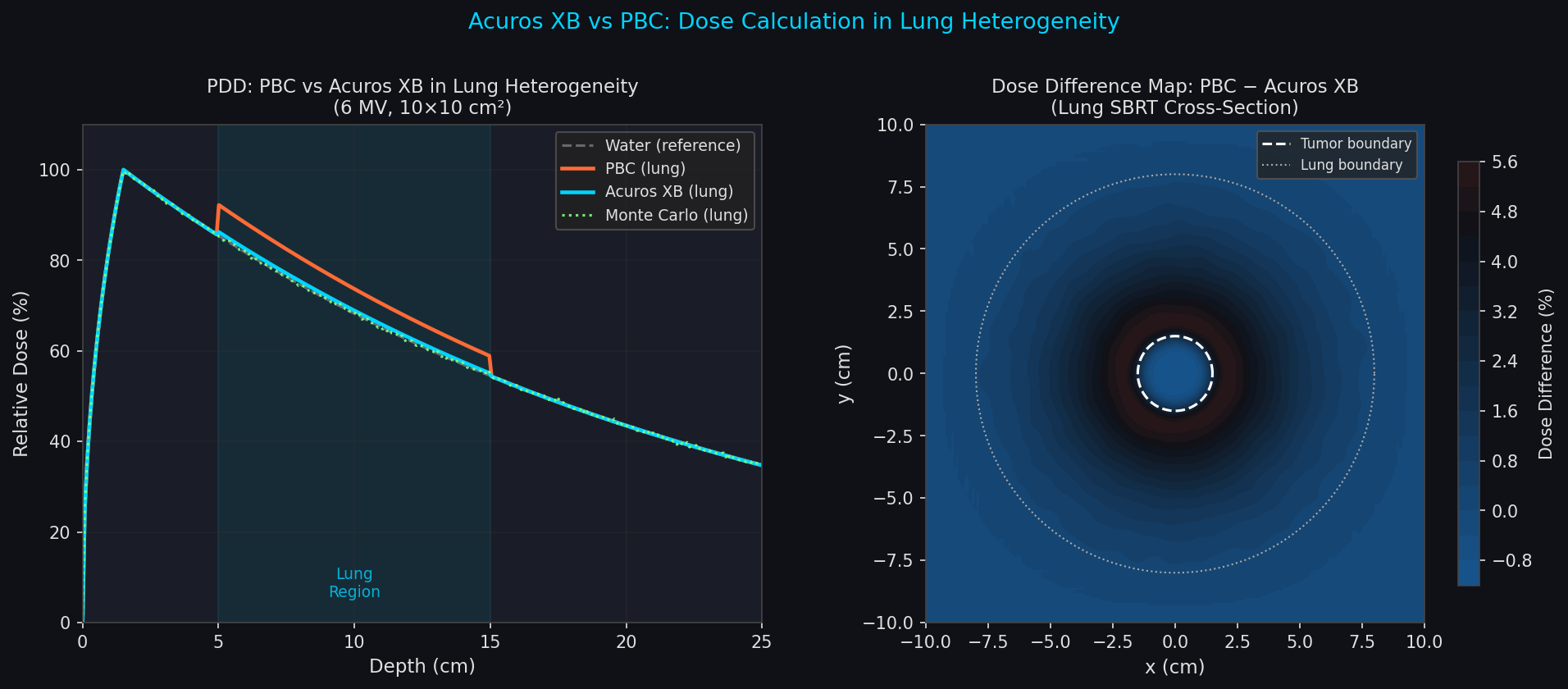
Conventional pencil-beam convolution (PBC) algorithms approximate photon scatter using pre-computed kernels derived from water-phantom measurements. In homogeneous tissue this works well, but accuracy degrades sharply at tissue interfaces—lung/soft-tissue boundaries, air cavities, bone, and metallic implants. Studies have shown PBC can overestimate dose in low-density lung tissue by 5–15%, a clinically significant error that can lead to tumor under-dosing or normal-tissue toxicity.
Monte Carlo (MC) methods solve this by tracking individual photon and electron histories through a voxelized patient CT geometry, sampling interaction probabilities from fundamental cross-section data. The result is the gold standard for heterogeneous media, but full MC requires millions of particle histories and can take hours per plan on clinical hardware.

Acuros XB: Deterministic Transport as a Monte Carlo Surrogate
Acuros XB solves the LBTE directly on the patient CT grid, computing the angular fluence of photons and electrons at every voxel without stochastic sampling. Key implementation details:
- Material assignment: CT Hounsfield Units are mapped to a library of biological materials (water, lung, cortical bone, adipose, muscle) with tabulated mass energy-absorption coefficients. This is more physically rigorous than the water-equivalent density scaling used by PBC.
- Spatial discretization: The patient volume is divided into a Cartesian mesh (typically 1–3 mm voxels). Fluence is expanded in a discrete-ordinates angular quadrature set (S8 or S12), balancing angular resolution against computation time.
- Source model: A beam-commissioning phase characterizes the linac's photon fluence spectrum, off-axis softening, and multi-leaf collimator (MLC) transmission. This source model feeds directly into the LBTE boundary conditions.
- Dose reporting modes: Acuros XB can report dose-to-medium (Dm,m) or dose-to-water-in-medium (Dw,m). The distinction matters for plan comparison with MC codes and for radiobiological modeling—Dm,m is the physically correct quantity, while Dw,m facilitates comparison with ion-chamber measurements calibrated in water.
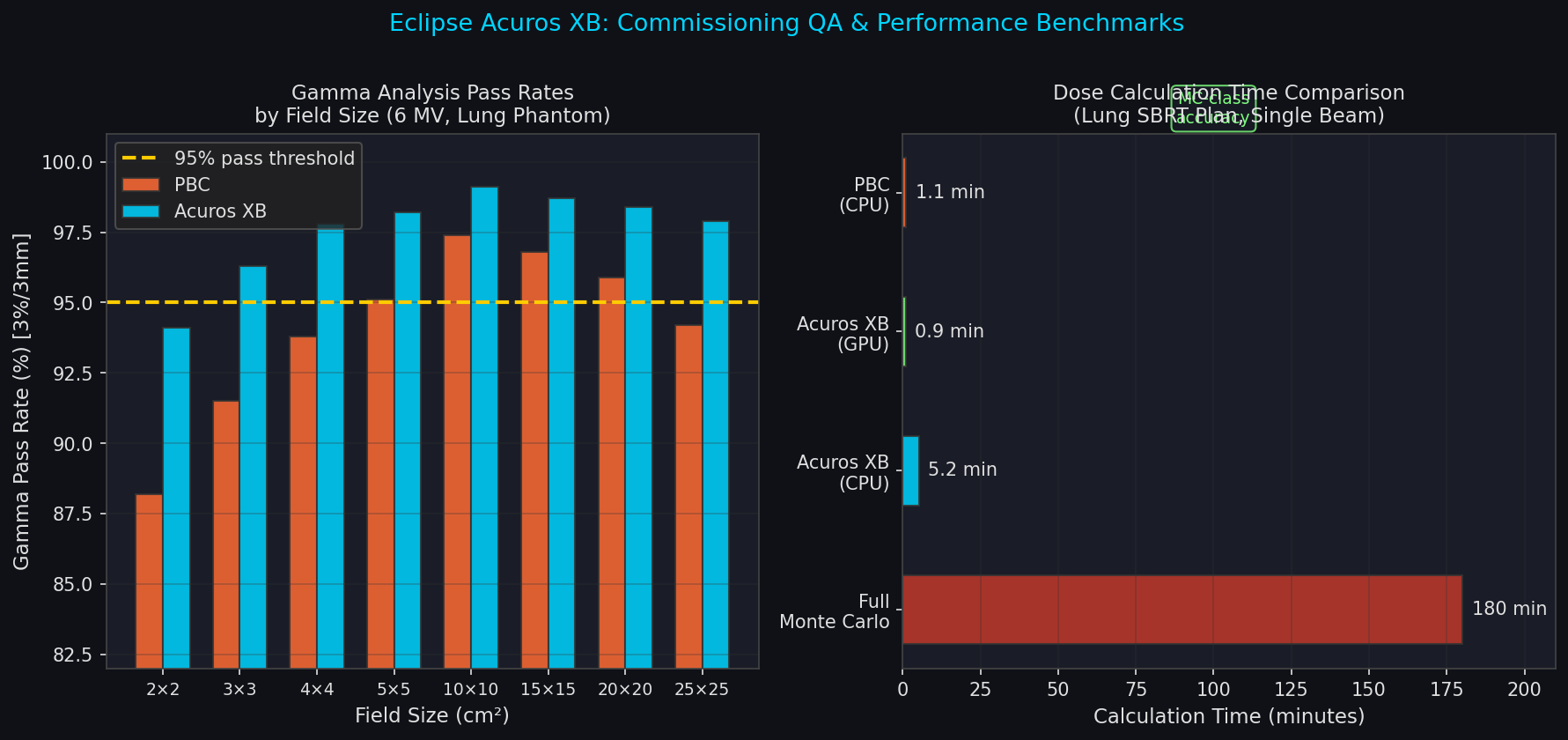
Benchmark studies comparing Acuros XB against full MC codes (EGSnrc, GEANT4) in lung SBRT and head-and-neck cases consistently show agreement within 1–2% in high-dose regions and within 2–3% in penumbra zones—performance indistinguishable from MC for clinical purposes, at computation times of 2–5 minutes per beam on a modern GPU workstation.
Clinical Workflow: Lung SBRT as a Case Study
Stereotactic Body Radiation Therapy (SBRT) for early-stage non-small cell lung cancer (NSCLC) is the scenario where algorithm choice has the greatest clinical impact. A typical Eclipse workflow proceeds as follows:
-
CT simulation and contouring: A 4D-CT acquisition captures tumor motion across the breathing cycle. The radiation oncologist contours the Internal Target Volume (ITV) on a maximum-intensity projection (MIP) image, then adds a Planning Target Volume (PTV) margin. Organs at risk (OARs)—spinal cord, esophagus, brachial plexus, chest wall—are also delineated.
-
Beam arrangement: A non-coplanar arc or static-field arrangement is designed to concentrate dose at the PTV while distributing entrance/exit dose across multiple beam paths. Eclipse's Photon Optimizer (PO) or Progressive Resolution Optimizer (PRO) handles fluence map optimization for IMRT/VMAT plans.
-
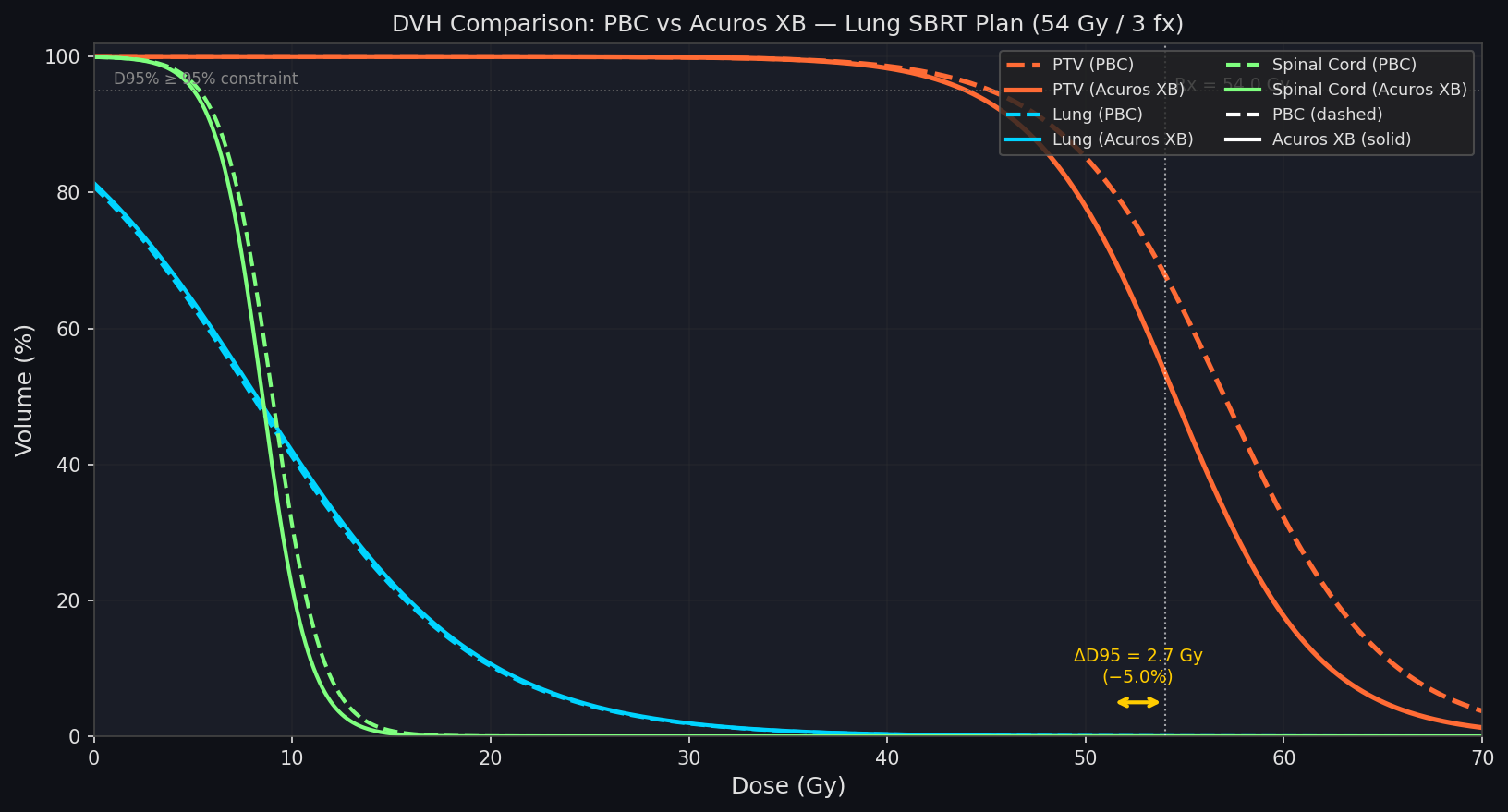
Acuros XB dose calculation: With the optimized fluence map, Acuros XB computes the 3D dose distribution. For a 54 Gy / 3-fraction SBRT plan, the planner verifies:
- PTV D95% ≥ 95% of prescription dose
- PTV D99% ≥ 90%
- Spinal cord Dmax < 18 Gy (3-fraction constraint)
- Chest wall V30Gy < 30 cc
-
Plan evaluation and DVH analysis: Eclipse's Dose-Volume Histogram (DVH) tools display cumulative and differential DVH curves for all structures. The Biological Evaluation module can compute Equivalent Uniform Dose (EUD) and Tumor Control Probability (TCP) using the linear-quadratic model, enabling radiobiological plan comparison.
-
Secondary check: Independent dose verification using a second algorithm (e.g., RadCalc or 3DVH) or measurement-based QA (ArcCHECK phantom) is performed before treatment delivery.
Heterogeneity Correction: Quantifying the PBC vs. Acuros XB Difference
For a representative lung SBRT case (2 cm tumor, 400 HU surrounding lung), switching from PBC to Acuros XB typically produces:
| Metric | PBC | Acuros XB | Difference |
|---|---|---|---|
| PTV D95% | 54.0 Gy | 51.3 Gy | −4.9% |
| PTV Dmax | 61.2 Gy | 60.8 Gy | −0.7% |
| Lung V20Gy | 4.1% | 4.3% | +0.2% |
| Spinal cord Dmax | 8.4 Gy | 8.1 Gy | −3.6% |
The PTV D95% drop of ~5% when switching to Acuros XB is clinically significant: a plan that appeared adequate under PBC may require re-optimization to meet coverage constraints. Many institutions now mandate Acuros XB for all thoracic SBRT cases.
GPU Acceleration and Adaptive Radiotherapy
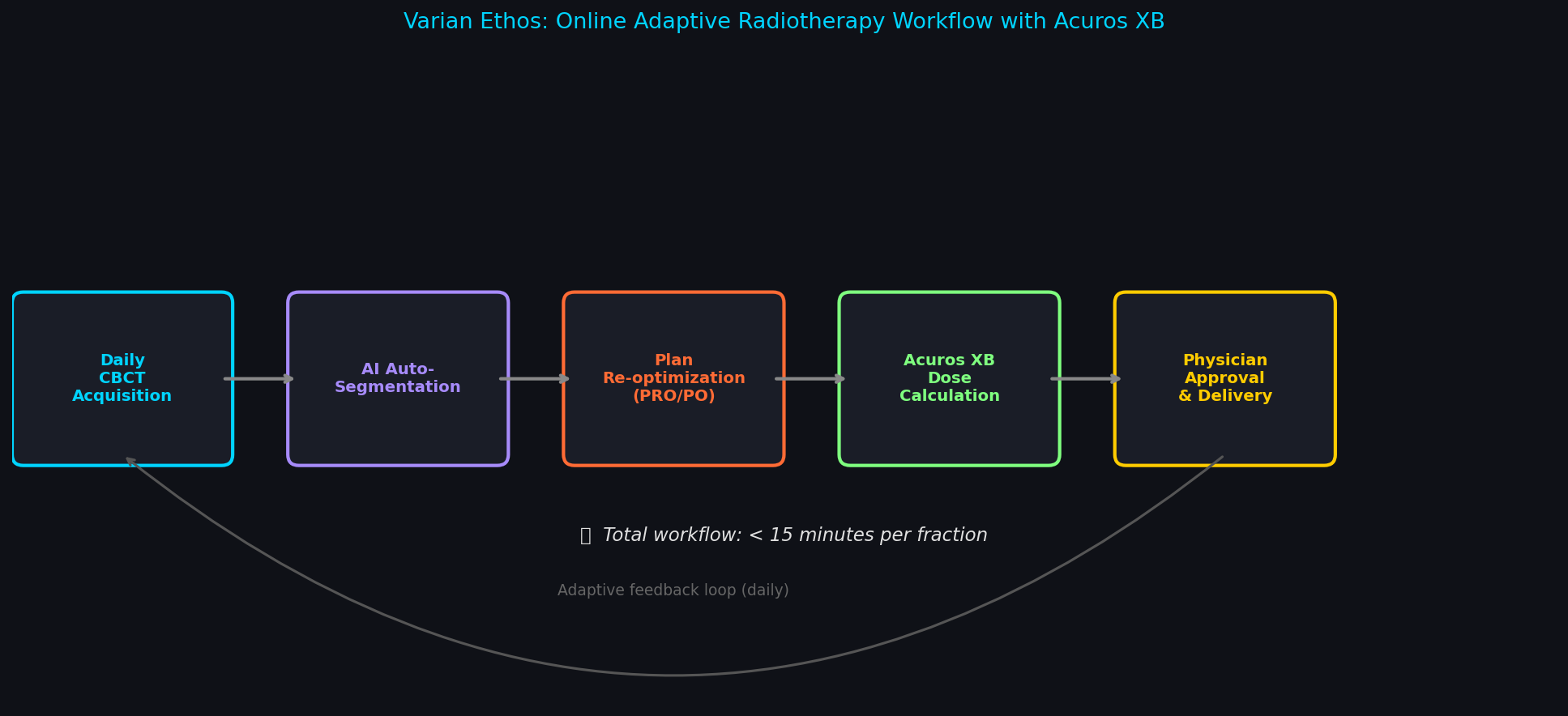
Eclipse 16+ integrates NVIDIA GPU acceleration for Acuros XB, reducing per-plan calculation times from ~5 minutes (CPU) to under 60 seconds on a workstation with a modern GPU. This speed enables online adaptive radiotherapy (ART) workflows, where the plan is recalculated on a daily cone-beam CT (CBCT) to account for anatomical changes—tumor shrinkage, weight loss, organ filling variation—and re-optimized before each fraction.
The Ethos adaptive therapy system from Varian automates this loop: CBCT acquisition → AI-driven auto-segmentation → plan re-optimization → Acuros XB dose calculation → physician approval → delivery, all within a 15-minute treatment slot.
Commissioning and Validation Requirements
Before clinical use, Acuros XB requires a rigorous commissioning process per AAPM Task Group 114 (TG-114) and TG-244 guidelines:
- Beam data acquisition: Percentage depth dose (PDD) curves, cross-beam profiles, and output factors measured in a water phantom for all field sizes and energies.
- Heterogeneity phantom measurements: Dose measured in a lung-equivalent phantom (e.g., CIRS ATOM) to validate algorithm performance at tissue interfaces.
- End-to-end testing: An anthropomorphic phantom irradiated with a clinical-like plan, with film and ion-chamber measurements compared against Eclipse predictions. Gamma analysis (3%/3mm criterion) pass rates >95% are typically required.
Further Resources
- Varian Eclipse TPS Product Page
- Acuros XB Algorithm Reference Guide (Varian)
- AAPM TG-114: Verification of Monitor Unit Calculations for Non-IMRT Clinical Radiotherapy
- Vassiliev et al., "Validation of the Acuros XB dose calculation algorithm," Medical Physics, 2010
- Fogliata et al., "Dosimetric evaluation of Acuros XB Advanced Dose Calculation algorithm in heterogeneous media," Radiation Oncology, 2011